The Research: ED precedes coronary artery disease symptoms by
2–3 years and a heart attack or stroke by
3–5 years on average. Men with ED have
more than double the rate of heart attacks, strokes, and cardiovascular death vs. men without ED (AHA Circulation, 1,900 men, avg age 69). This window is your opportunity — not just a warning.
 Connection Connection |  What the Research Shows What the Research Shows |  Why This Happens Why This Happens |  What to Do What to Do |
|---|
| ED → Heart Attack / Stroke Risk | +43% CVD risk
+59% coronary heart disease
+34% stroke risk
+33% all-cause mortality
(Meta-analysis, ~155,000 men) | Same endothelial dysfunction damages both penile arteries (1–2mm) and coronary arteries (3–4mm). Penile arteries show damage first due to smaller diameter. | Request comprehensive cardiovascular evaluation from your doctor — blood pressure, fasting lipids, fasting glucose, BMI — even without other symptoms. |
| Timing: ED → CAD Symptoms | 2–3 years earlier
ScienceDirect meta-analysis | In 2 out of 3 men with proven coronary artery disease, ED appeared first — an average of 39 months before the first episode of chest pain. | Treat new, consistent ED after 60 as a cardiovascular signal. Don’t wait for chest pain to seek evaluation. |
| Timing: ED → Heart Attack | 3–5 years earlier
Multiple studies, ACC guidelines | This 3–5 year window is a preventive opportunity. Lifestyle intervention during this period can reverse endothelial damage and reduce cardiac risk. | Begin aerobic exercise (30 min daily), Mediterranean diet, and address blood pressure and blood sugar immediately. |
| Severity of ED | Dose-response: more severe ED = higher cardiovascular risk | The severity of erectile dysfunction correlates with the severity of coronary artery disease. Mild ED = early signal. Consistent, complete inability = stronger signal. | Worsening or consistent ED warrants more urgent evaluation than occasional difficulty. Discuss severity specifically with your doctor. |
| 2024 Princeton IV Guidelines | “ED is a vital sign for cardiovascular health” — Mayo Clinic summary | ACC/AHA guidelines now classify ED as a risk-enhancing factor for atherosclerotic cardiovascular disease (ASCVD), particularly for silent coronary artery disease. | Bring up ED explicitly at your next doctor’s visit and ask for your ASCVD risk score to be calculated. |
| Shared Risk Factors | Hypertension, diabetes, obesity, low testosterone, inflammation, smoking — all drive both conditions | These risk factors all damage endothelial function and reduce nitric oxide production — the common pathway for both ED and cardiovascular disease. | Addressing any one risk factor improves both conditions simultaneously. Exercise, diet, and weight loss work on all pathways at once. |
The opportunity: ED gives you a 3–5 year head start on preventing a potential cardiac event. Men who respond to new ED with cardiovascular evaluation, daily exercise, diet improvement, and blood pressure management are practicing the most impactful form of preventive medicine available. Do not wait for chest pain.
Sources: AHA Circulation (2018, 1,900 men avg age 69) — 2× cardiovascular death/MI/stroke rate with ED · Meta-analysis ~155,000 men — 43% CVD, 59% CHD, 34% stroke, 33% all-cause mortality increase · ScienceDirect — ED precedes CAD 2–3 yrs, cardiac events 3–5 yrs · Princeton IV Consensus Guidelines (J Sex Med 2024) — ED as ASCVD risk-enhancing factor · Mayo Clinic 2025 — ED as cardiovascular vital sign · Brown University Health — vasculogenic ED and the 3–5 year window · Montorsi study (300 men, angiographically proven CAD) — 39 months from ED to first chest pain
Most men who experience erectile dysfunction after 60 think of it as a quality-of-life issue.
The medical community increasingly thinks of it as something else entirely: an early warning system for the heart.
In 2018, a landmark study published in the American Heart Association journal Circulation followed nearly 2,000 racially diverse men — average age 69 — who had no prior history of heart disease or stroke. After four years, men with erectile dysfunction had experienced more than twice the rate of heart attacks, strokes, and cardiovascular death compared to men without ED: 6.3 percent versus 2.6 percent.
This association held up after controlling for every traditional cardiovascular risk factor — blood pressure, cholesterol, diabetes, smoking, age. The connection between ED and heart disease was independent.
“It is incredible how many men avoid the doctor, and avoid early signs of cardiovascular disease, but present for the first time with a chief complaint of ED,” said Dr. Michael Blaha, the study’s senior author and director of clinical research at the Johns Hopkins Ciccarone Center for the Prevention of Heart Disease.
This post explains why this connection exists, what the research says about timing, and exactly what men over 60 should do when ED first appears.
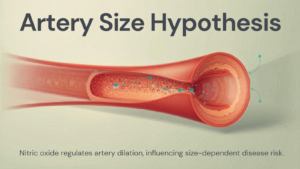
Why Erectile Dysfunction Appears Before Heart Disease — The Artery Size Hypothesis
The explanation for why ED precedes cardiovascular events is well established in cardiology and is known as the artery size hypothesis.
Erections depend entirely on blood flow. When the brain sends arousal signals, the endothelial cells lining penile blood vessels produce nitric oxide, which relaxes and dilates those vessels, allowing blood to fill the erectile tissue.
The penile artery is approximately 1 to 2 millimeters in diameter. The coronary arteries supplying the heart are approximately 3 to 4 millimeters. Both are damaged by the same underlying process: endothelial dysfunction and atherosclerosis — the buildup of plaque that stiffens and narrows arterial walls.
Because the penile artery is smaller, it reaches the threshold of functionally compromised blood flow earlier than the coronary arteries. The same degree of systemic arterial damage that blocks enough blood flow to the penis to cause ED has not yet blocked enough flow to the heart to cause chest pain or a cardiac event.
In other words: the penis reports the problem before the heart does.
ScienceDirect research puts the timing precisely: ED precedes clinically evident coronary artery disease by 2 to 3 years, and precedes a cardiovascular event — heart attack or stroke — by 3 to 5 years on average.
That window is not a problem. It is an opportunity.
What the Research Shows: The Numbers Are Stark
The 2018 AHA Circulation study is one of dozens now supporting this link. A meta-analysis incorporating data from nearly 155,000 men produced the following findings for men with ED compared to men without:
- 43% increased cardiovascular disease risk overall
- 59% increased coronary heart disease risk
- 34% increased stroke risk
- 33% increased all-cause mortality risk
In 2024, the American College of Cardiology and the Princeton IV Consensus Guidelines — the definitive cardiology guidance on ED and heart health — formally recommended that erectile dysfunction be treated as a risk-enhancing factor for cardiovascular disease, particularly for identifying silent coronary artery disease in men who have no other symptoms.
Mayo Clinic summarized the 2024 Princeton IV findings directly: ED should be treated as a vital sign for cardiovascular health.
In two-thirds of men with angiographically proven coronary artery disease, ED symptoms appeared first — an average of 39 months before the first episode of chest pain.
How Severe the ED Is Matters — The Dose-Response Relationship
One of the most important findings across multiple studies is that the relationship between ED severity and cardiovascular risk is not binary — it follows a dose-response pattern.
The more severe the erectile dysfunction, the greater the risk of ischemic heart disease, heart failure, peripheral vascular disease, and all-cause mortality.
This means occasional mild difficulty is a different signal than consistent inability to achieve or maintain an erection. Both warrant a cardiovascular conversation with your doctor. But consistent, worsening ED in a man over 60 is the stronger signal and the more urgent one.
For men aged 40 to 49 with a new diagnosis of ED not related to secondary causes — medications, psychological factors, injury — research found a nearly 50-fold increase in coronary artery disease incidence over 10 years. The signal is most dramatic in younger men, but it persists at every age including well past 60.
What Shared Risk Factors Connect ED and Heart Disease?
ED and cardiovascular disease share the same underlying biology and the same modifiable risk factors. Understanding this is what makes the ED-as-warning-sign framework actionable rather than just alarming.
Endothelial Dysfunction
The endothelium — the inner lining of blood vessels — is the common target. When endothelial cells stop producing nitric oxide efficiently, blood vessels lose their ability to dilate on demand. This affects the penile artery first, the coronary arteries shortly after.
Hypertension
High blood pressure damages arterial walls and accelerates plaque formation in both penile and coronary arteries. Men with hypertension are significantly more likely to develop ED, and the ED, in turn, signals that arterial damage is already underway.
Type 2 Diabetes
Among men with diabetes, ED prevalence is approximately 51 percent — more than double the general population rate. Diabetes damages both the vascular system and the nerve pathways involved in arousal, compounding the ED risk.
Obesity and Visceral Fat
Abdominal obesity drives insulin resistance, suppresses testosterone, and promotes systemic inflammation — all of which damage endothelial function and raise both ED and cardiovascular risk simultaneously.
Low Testosterone
Testosterone decline that accelerates after 60 contributes directly to ED through reduced libido and impaired vascular function. Low testosterone is also an independent predictor of cardiovascular events.
Chronic Inflammation
The same low-grade chronic inflammation that drives cardiovascular disease also damages the endothelial cells responsible for nitric oxide production. The anti-inflammatory diet addresses both pathways simultaneously.
What to Do When ED First Appears After 60: The 5-Step Response
The 3 to 5 year window between ED onset and cardiovascular event is the most important number in this entire conversation. It means that acting on ED as a cardiovascular warning when it first appears is genuinely preventive medicine.
Step 1: See Your Doctor — Specifically for Cardiovascular Evaluation
Not just for the ED. For your heart.
The ACC Princeton IV guidelines specifically recommend that men presenting with ED receive a comprehensive cardiovascular risk assessment — blood pressure, fasting lipids, fasting glucose, BMI, and family history. If elevated risk is found, additional cardiac testing is indicated.
Many men with early cardiovascular disease have no chest pain, no shortness of breath, and no other symptoms. ED may be the only signal their body is sending.
Step 2: Address the Modifiable Risk Factors Directly
Every risk factor shared by ED and cardiovascular disease is modifiable. Blood pressure, cholesterol, blood sugar, body weight, activity level, and diet are all within your control.
Research published in the Journal of Sexual Medicine found that aerobic exercise — specifically 40 minutes of moderate activity four times per week over six months — improved erectile function scores to a degree comparable to medication in some men. It works through the same nitric oxide and vascular health pathways that exercise uses to protect the heart.
Step 3: Start Walking Every Day
A Harvard study of over 22,000 men found that 30 minutes of brisk walking daily was linked to a 41 percent lower risk of ED. The same daily walking routine that protects erectile function is also the single most accessible cardiovascular intervention available.
Zone 2 walking — at a pace where you can speak in full sentences but feel your heart working — is where the most significant improvements in endothelial health and nitric oxide production occur. The Japanese walking method and the 12-3-30 treadmill approach are both effective structured formats to build this into a daily routine.
Step 4: Overhaul Your Diet
The dietary pattern with the strongest evidence for both erectile function and cardiovascular protection is the Mediterranean diet — centered on anti-inflammatory foods: fatty fish, leafy greens, olive oil, nuts, berries, and legumes.
A 10-year study of over 25,000 men found that those eating flavonoid-rich foods were significantly less likely to develop ED. The same foods that reduce cardiovascular inflammation are the same ones that protect endothelial function in penile arteries. See our list of the 5 daily longevity foods with the strongest evidence for senior health.
Step 5: Reduce the Specific Lifestyle Drivers
Three lifestyle factors significantly worsen both ED and cardiovascular risk and can be addressed directly:
- Smoking — constricts blood vessels, accelerates endothelial damage, reduces nitric oxide production. Quitting is the single most impactful vascular intervention available.
- Heavy alcohol consumption — regular drinking above 2 units daily suppresses testosterone, damages blood vessel walls, and impairs the nitric oxide pathway.
- Chronic sleep deprivation — testosterone is produced primarily during deep sleep. Poor sleep raises cortisol, suppresses testosterone, and accelerates the vascular damage that underlies both ED and heart disease.
ED After 60: What Is Normal Aging vs. What Is a Red Flag?
Not every change in erectile function after 60 is a cardiovascular alarm. Understanding the distinction matters.
Normal Age-Related Changes
After 60, it is normal for erections to take longer to achieve, require more direct stimulation, and feel somewhat less firm than at 40. Refractory periods — the recovery time between erections — lengthen with age. These are expected physiological changes, not disease signals.
Patterns That Warrant Cardiovascular Investigation
- Consistent inability to achieve or maintain an erection sufficient for sexual activity — not occasional difficulty
- A noticeable change in function that developed over weeks or months rather than gradually over years
- ED appearing alongside other new symptoms: unusual fatigue during mild exertion, leg pain when walking, shortness of breath that was not present before
- ED in a man with known risk factors — hypertension, diabetes, elevated cholesterol, obesity, smoking history — even without other cardiac symptoms
The key question is not whether ED is present — it is whether it represents a change from your previous baseline and whether it is consistent rather than occasional.
Our full guide on what is actually happening in erections over 60 covers the complete picture of age-related changes, vascular causes, hormonal contributors, and what the research says about each treatment approach.
Frequently Asked Questions
Is erectile dysfunction always a sign of heart disease?
No — but it is a signal that warrants cardiovascular evaluation, especially in men over 60. ED can have psychological, hormonal, neurological, and medication-related causes that are not cardiovascular. However, the most common cause of ED in men over 60 is vascular — impaired blood flow caused by the same endothelial dysfunction that underlies heart disease. The 2024 Princeton IV Consensus Guidelines recommend every man with ED receive a cardiovascular risk assessment, regardless of other symptoms.
How long before a heart attack does erectile dysfunction appear?
Research consistently finds that ED symptoms appear 2 to 3 years before clinically evident coronary artery disease, and 3 to 5 years before a cardiovascular event such as a heart attack or stroke. In a study of 300 men with proven coronary artery disease, two-thirds experienced ED symptoms an average of 39 months before their first episode of chest pain.
What percentage of men with ED have heart disease?
Studies show that ED affects 43.8% of men aged 60 to 69 and up to 70% of men over 70. Among men presenting with ED, research finds that up to 30% show evidence of previously undetected cardiovascular disease when properly evaluated. A meta-analysis of nearly 155,000 men found ED was associated with a 43% increased overall cardiovascular disease risk.
Should I see a cardiologist if I have erectile dysfunction?
Start with your primary care physician and request a comprehensive cardiovascular risk assessment — blood pressure, fasting lipids, fasting glucose, BMI, and family history review. If traditional risk factors are elevated, or if you have additional symptoms, your doctor may refer you to a cardiologist for further testing. Do not delay the initial evaluation. The 3 to 5 year window between ED onset and cardiac events is the opportunity to intervene before anything serious occurs.
Can fixing erectile dysfunction improve heart health?
Lifestyle changes that improve erectile function work through the same vascular mechanisms that protect heart health — they are not separate interventions. Regular aerobic exercise, a Mediterranean-style diet, weight reduction, smoking cessation, and blood pressure control all simultaneously improve endothelial function, nitric oxide production, and arterial flexibility in both penile and coronary arteries. Treating ED as the cardiovascular wake-up call it is, and responding with real lifestyle change, is genuinely protective.
Does Viagra or Cialis protect against heart disease?
The 2024 Princeton IV Consensus Guidelines note that PDE5 inhibitors — including sildenafil (Viagra) and tadalafil (Cialis) — have a potential cardioprotective role and are generally safe even in men with stable cardiovascular disease or risk factors. Some research suggests these medications may have additional vascular benefits beyond treating ED. However, they are not a substitute for cardiovascular evaluation or lifestyle modification when ED appears as a warning sign.
Conclusion
There is a phrase that cardiologists use for erectile dysfunction: the canary in the coalmine.
It appears before the more dangerous event. It does so reliably. And it gives you a window of years to act.
A man over 60 who experiences consistent erectile dysfunction and responds by getting a cardiovascular evaluation, starting a daily walking routine, overhauling his diet, and addressing his blood pressure and blood sugar is not just managing a sexual health issue.
He is potentially preventing a heart attack.
That is what the research says. That is what the 2024 Princeton IV Consensus Guidelines say. That is what Johns Hopkins, the American Heart Association, and Mayo Clinic all say.
The 3 to 5 year window is the most important number in this article. Do not wait for chest pain. The daily habits that protect the heart are the same ones that protect erectile function — and the longevity research points to the same lifestyle changes from every direction.